Renal Cell Carcinoma
Comprehensive treatment for kidney cancer, including surgery, immunotherapy, and targeted therapy.
Renal Cell Carcinoma
Solid Tumors
Overview
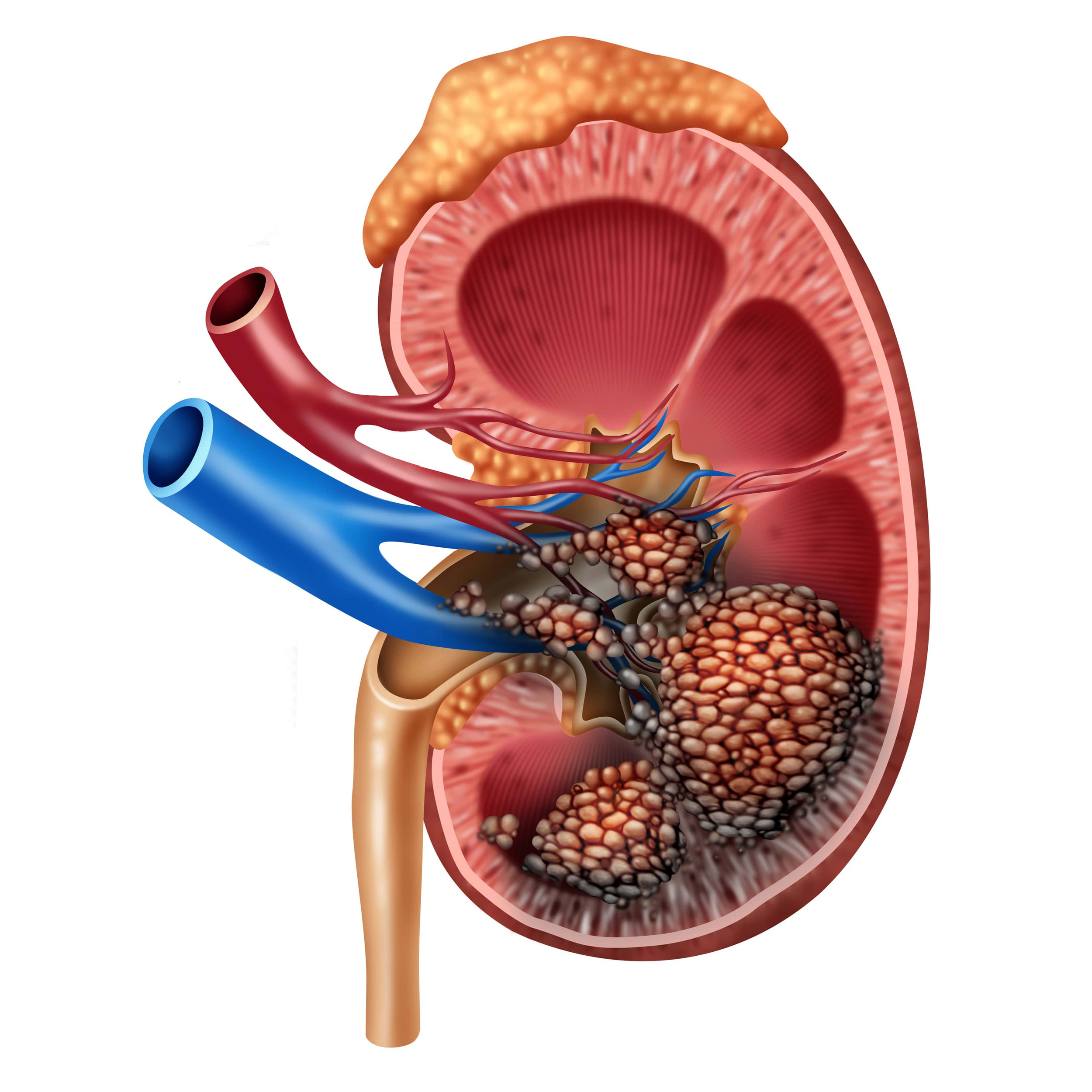
Renal Cell Carcinoma (RCC), or kidney cancer, is a major urological malignancy originating in the lining of the proximal convoluted tubules—the tiny tubes in the kidneys that filter waste from the blood and produce urine. RCC accounts for approximately 90% of all kidney cancers. The disease is histologically classified into several subtypes, with Clear Cell RCC being the most common (about 70-80% of cases), followed by Papillary RCC (about 10-15%) and Chromophobe RCC (about 5%).
Clear cell RCC is characterized by cells with clear cytoplasm and is highly vascularized, driven by genetic pathways related to the Von Hippel-Lindau (VHL) gene. RCC is associated with several risk factors, including smoking (which doubles the risk), obesity, hypertension, chronic kidney disease, dialysis, and genetic syndromes like VHL disease and Birt-Hogg-Dubé syndrome. Early-stage RCC is typically asymptomatic and is frequently detected incidentally during abdominal imaging performed for unrelated symptoms (known as 'incidentalomas').
When symptoms do occur, they represent advanced or locally invasive disease. The classic triad of RCC symptoms includes blood in the urine (hematuria), flank pain, and a palpable abdominal mass, although all three are present in only about 10% of patients. Other symptoms include unexplained weight loss, fatigue, persistent fever, night sweats, anemia, and paraneoplastic syndromes (such as hypercalcemia or erythrocytosis) caused by tumor hormone secretion.
When to Consult
After diagnosis of kidney cancer, detection of kidney mass, blood in urine, flank pain, or unexplained weight loss.
What to Bring
CT/MRI scans, biopsy reports, blood test results including kidney function tests, genetic testing results (VHL, MET), and family history.
Risk Factors
Causes
Treatment Options
Partial Nephrectomy (Nephron-Sparing Surgery)
Partial nephrectomy, or nephron-sparing surgery, is the gold standard surgical treatment for localized, early-stage Renal Cell Carcinoma (typically tumors <= 4 cm, Stage T1a, and selected T1b tumors up to 7 cm). The procedure involves removing the kidney tumor along with a minimal margin of surrounding healthy tissue, leaving the rest of the kidney intact. The primary goal is to preserve maximum kidney function, which reduces the long-term risk of chronic kidney disease and cardiovascular complications. Partial nephrectomy is performed using open, laparoscopic, or robot-assisted techniques, with robotic surgery offering superior precision and visualization for complex tumor reconstructions.
Radical Nephrectomy
Radical nephrectomy is a surgical procedure that involves the complete removal of the affected kidney, the surrounding perinephric fat, Gerota's fascia, and regional lymph nodes, sometimes accompanied by removal of the adjacent adrenal gland if it is involved. It is indicated for large renal tumors (Stage T2 or greater), tumors located centrally in the kidney, or when a partial nephrectomy is not technically feasible due to tumor anatomy. Radical nephrectomy can also be performed laparoscopically or robotically. In cases where the tumor has invaded the renal vein or inferior vena cava, a complex surgery involving vascular reconstruction is performed to extract the tumor thrombus.
Local Ablative and Minimally Invasive Therapies
For patients with small renal masses (typically <= 3 cm) who are elderly, have significant comorbidities, or are otherwise poor candidates for major surgery, minimally invasive ablative therapies are highly effective alternatives. These include Cryoablation, which uses extreme cold delivered via probes to freeze and destroy the tumor tissue, and Radiofrequency Ablation (RFA), which uses electrical currents to heat and destroy cells. These procedures are performed percutaneously under local anesthesia and CT or ultrasound guidance. Active Surveillance is also a valid option for small, slow-growing tumors in patients with limited life expectancy, involving monitoring with regular ultrasounds or CT scans.
Doublet Immunotherapy and TKI-IO Combinations
For advanced or metastatic Renal Cell Carcinoma, systemic therapy has undergone a paradigm shift, moving away from cytotoxic chemotherapy (which is ineffective in RCC) to combinations of immunotherapy and targeted therapy . First-line treatments for metastatic clear cell RCC are determined by the IMDC risk category. For intermediate and poor-risk patients, doublet immunotherapy with Nivolumab (anti-PD-1) and Ipilimumab (anti-CTLA-4) is the standard. Alternatively, combinations of an immunotherapy checkpoint inhibitor and a VEGF-targeted tyrosine kinase inhibitor (TKI-IO) are used for all risk groups. Examples include Pembrolizumab plus Axitinib, Lenvatinib plus Pembrolizumab, or Cabozantinib plus Nivolumab.
Targeted Tyrosine Kinase Inhibitors (TKI) and mTOR Inhibitors
Targeted therapies are designed to block pathways involved in angiogenesis and cell growth, which are highly active in RCC due to VHL gene inactivation. Tyrosine kinase inhibitors (TKIs) targeting the Vascular Endothelial Growth Factor (VEGF) receptors are widely used as monotherapy or in combination. These oral medications include Sunitinib, Pazopanib, Cabozantinib, and Axitinib, which inhibit tumor blood vessel formation. Additionally, mTOR inhibitors such as Everolimus and Temsirolimus target the mammalian target of rapamycin pathway. Recently, Belzutifan, a targeted inhibitor of HIF-2alpha, has been approved for patients with VHL-associated RCC and advanced clear cell RCC.
Frequently Asked Questions
Q. What is the most effective treatment for Renal Cell Carcinoma?
The most effective treatment for Renal Cell Carcinoma depends on the stage, location, molecular profile of the tumor, and the patient's overall health. Dr. R. Srinath Bharadwaj provides personalized protocols including chemotherapy , immunotherapy , targeted therapy , or combination approaches.
Q. Where can I get expert treatment for Renal Cell Carcinoma in Hyderabad?
You can consult Dr. R. Srinath Bharadwaj, a leading Medical Oncologist, at the American Oncology Institute, Nallagandla, Hyderabad. Call +91 91213 36638 to schedule an appointment.
Q. What documents should I bring for a Renal Cell Carcinoma consultation?
Please bring all recent biopsy reports, imaging scans (CT, MRI, or PET-CT), tumor markers, blood test results, and any previous treatment or surgery details to help outline your care plan.