Pancreatic Cancer
Comprehensive treatment for pancreatic cancer including surgery (Whipple procedure), chemotherapy, targeted therapy, and radiation therapy.
Pancreatic Cancer
Solid Tumors
Overview
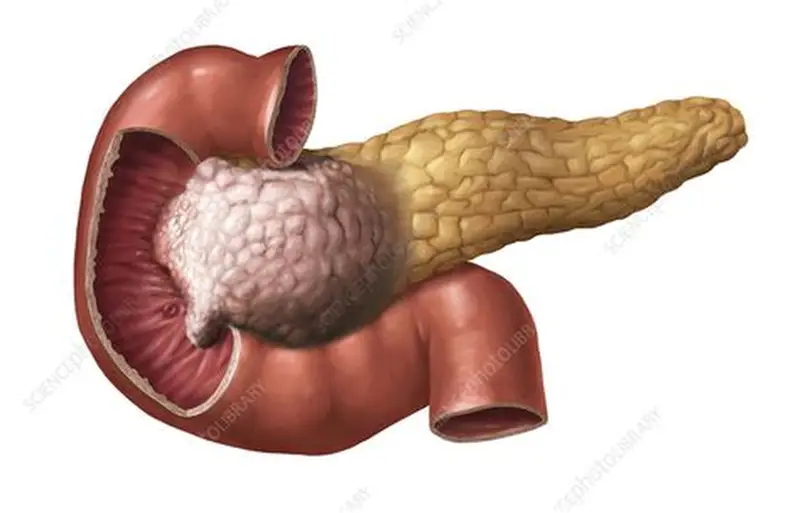
Pancreatic cancer is one of the most lethal and aggressive malignancies, characterized by rapid progression, early metastatic spread, and a poor prognosis. It arises from the tissues of the pancreas—a retroperitoneal gland located behind the stomach that plays crucial roles in digestion (exocrine function) and blood sugar regulation (endocrine function). Over 95% of pancreatic cancers are exocrine tumors, specifically Pancreatic Ductal Adenocarcinoma (PDAC), which originates in the cells lining the pancreatic ducts.
The remaining minority includes pancreatic neuroendocrine tumors (PNETs). PDAC is characterized by a dense, fibrous tissue reaction (desmoplasia) surrounding the tumor, which acts as a barrier to drug delivery. Tumors in the head of the pancreas (about 60-70% of cases) tend to present earlier due to obstruction of the common bile duct, causing jaundice.
Tumors in the body or tail are usually asymptomatic until advanced. Symptoms include painless or painful jaundice (dark urine, pale stools, yellowing of skin), significant unexplained weight loss, persistent mid-back or upper abdominal pain that worsens after eating or lying down, new-onset or worsening Type 2 diabetes, loss of appetite, nausea, vomiting, and fatigue. By the time symptoms prompt evaluation, the vast majority of patients have locally advanced or metastatic disease, with common sites of spread being the liver, peritoneum, lungs, and distant lymph nodes.
When to Consult
Upon diagnosis of pancreatic cancer, jaundice, unexplained weight loss, abdominal pain, back pain, or abnormal pancreatic imaging.
What to Bring
CT/MRI scans, endoscopic ultrasound reports, CA 19-9 blood test results, biopsy reports, genetic testing results (BRCA, PALB2), and previous treatment records.
Risk Factors
Causes
Treatment Options
Surgical Pancreaticoduodenectomy (Whipple Procedure)
For tumors located in the head of the pancreas, the Whipple procedure is the standard surgical intervention. This complex operation involves removing the head of the pancreas, the duodenum, the gallbladder, a portion of the common bile duct, and sometimes a part of the stomach. The surgeon then reconstructs the digestive tract by connecting the remaining pancreas, bile duct, and stomach to the small intestine (jejunum). The Whipple procedure is technically demanding and carries risks of complications such as pancreatic leaks, delayed gastric emptying, and infection, requiring an experienced hepatobiliary surgical team. Successful resection provides the only potential chance for long-term survival.
Distal Pancreatectomy and Total Pancreatectomy
For tumors located in the body or tail of the pancreas, a Distal Pancreatectomy is performed. This surgery involves removing the body and tail of the pancreas, and typically the spleen (splenectomy) due to its shared blood supply. Distal pancreatectomy can often be performed using minimally invasive laparoscopic or robotic techniques. A Total Pancreatectomy involves removing the entire pancreas, duodenum, spleen, gallbladder, and part of the stomach, but it is rarely performed. Total pancreatic resection results in the permanent loss of exocrine and endocrine functions, causing severe 'brittle' diabetes requiring lifelong insulin therapy and digestive enzyme replacements.
Neoadjuvant and Adjuvant Chemotherapy
Systemic chemotherapy is a critical component of pancreatic cancer care. For patients with resectable disease, adjuvant chemotherapy is administered post-surgery to reduce the high risk of recurrence. For patients with borderline resectable or locally advanced disease, neoadjuvant chemotherapy is given before surgery to shrink the tumor, improve the likelihood of a successful R0 resection, and treat early microscopic metastases. Standard regimens include FOLFIRINOX (a combination of 5-Fluorouracil, Leucovorin, Irinotecan, and Oxaliplatin) for fit patients, or the doublet of Gemcitabine and Nab-paclitaxel. These regimens are also used as the primary treatment for metastatic disease.
Targeted and Genetic-Based Therapies
Targeted therapies are playing an increasing role in pancreatic cancer as molecular profiling becomes routine. For patients with metastatic pancreatic cancer who harbor germline BRCA1 or BRCA2 mutations and whose disease has not progressed after platinum-based chemotherapy , the oral PARP inhibitor Olaparib is used as maintenance therapy to prolong progression-free survival. Small molecule inhibitors or monoclonal antibodies are utilized based on tumor markers. For the rare subset of patients with NTRK gene fusions, highly targeted agents like Larotrectinib or Entrectinib are available. Additionally, clinical trials are evaluating novel therapies targeting KRAS mutations, which are present in over 90% of pancreatic cancers.
Palliative Care and Symptom Management
Given the aggressive nature of pancreatic cancer, early integration of palliative and supportive care is vital to maintain quality of life. Key interventions include: biliary stent placement via ERCP to relieve jaundice caused by ductal obstruction; duodenal stent placement or surgical bypass (gastrojejunostomy) to relieve gastric outlet obstruction; Celiac Plexus Block, an injection of local anesthetic or alcohol to block nerve transmission and manage severe abdominal pain; Pancreatic Enzyme Replacement Therapy (PERT) to treat malabsorption and diarrhea caused by exocrine insufficiency; and nutritional counseling to manage weight loss and cachexia.
Frequently Asked Questions
Q. What is the most effective treatment for Pancreatic Cancer?
The most effective treatment for Pancreatic Cancer depends on the stage, location, molecular profile of the tumor, and the patient's overall health. Dr. R. Srinath Bharadwaj provides personalized protocols including chemotherapy , immunotherapy , targeted therapy , or combination approaches.
Q. Where can I get expert treatment for Pancreatic Cancer in Hyderabad?
You can consult Dr. R. Srinath Bharadwaj, a leading Medical Oncologist, at the American Oncology Institute, Nallagandla, Hyderabad. Call +91 91213 36638 to schedule an appointment.
Q. What documents should I bring for a Pancreatic Cancer consultation?
Please bring all recent biopsy reports, imaging scans (CT, MRI, or PET-CT), tumor markers, blood test results, and any previous treatment or surgery details to help outline your care plan.