Ovarian Cysts
Evaluation and management of ovarian cysts, including monitoring and treatment when necessary.
Ovarian Cysts
Solid Tumors
Overview
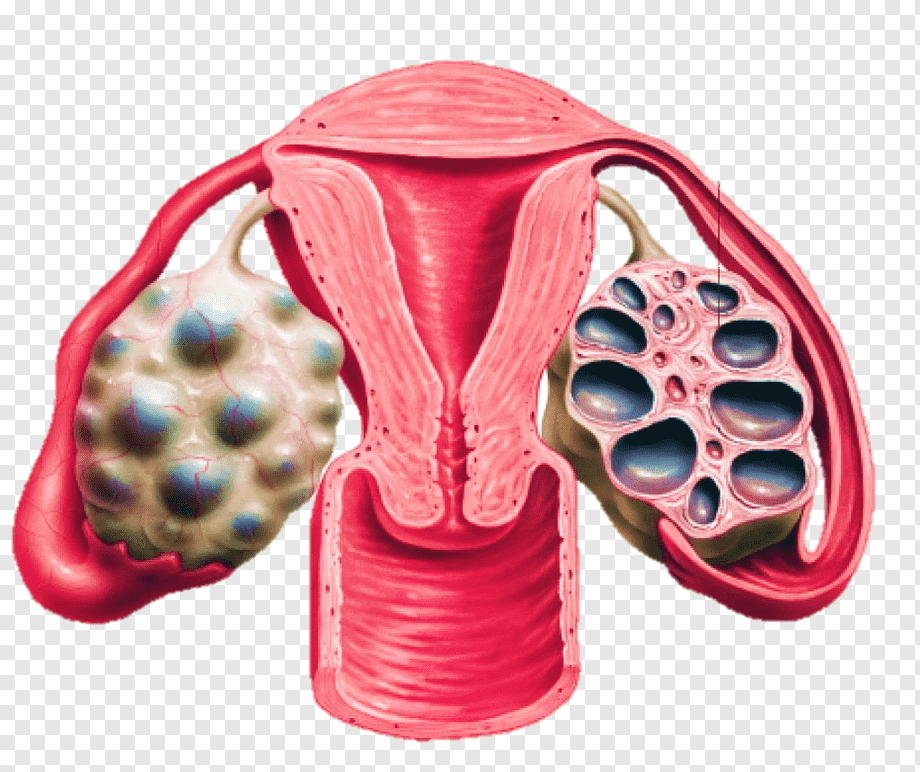
Ovarian cysts are fluid-filled sacs or pockets that develop within or on the surface of one or both ovaries, which are the almond-shaped female reproductive organs located in the pelvis that produce eggs (ova) and hormones (estrogen and progesterone). Ovarian cysts are extremely common and can develop at any stage of life, though they are most prevalent during a woman's childbearing years. The vast majority of ovarian cysts are benign, non-cancerous, and functional—meaning they develop as a normal part of the menstrual cycle.
Functional cysts include Follicular Cysts, which occur when a follicle fails to rupture and release its egg, and Corpus Luteum Cysts, which form when the sac seals after releasing the egg and accumulates fluid. These functional cysts typically resolve spontaneously within two to three menstrual cycles without treatment. Non-functional cysts include Endometriomas (caused by endometriosis, containing dark, old blood, often called 'chocolate cysts'), Dermoid Cysts or mature cystic teratomas (benign germ cell tumors containing tissues like hair, teeth, or fat), Cystadenomas (benign epithelial tumors that can grow very large), and malignant ovarian cysts (ovarian cancer).
Most ovarian cysts are small and asymptomatic, discovered incidentally during pelvic exams or ultrasounds. When symptoms do occur, they include dull or sharp pelvic pain (often on the side of the cyst), abdominal bloating or fullness, irregular menstrual periods, painful intercourse (dyspareunia), and urinary frequency. If a cyst ruptures or causes ovarian torsion (twisting of the ovary, blocking its blood supply), it presents as sudden, severe pelvic pain, nausea, and vomiting, requiring emergency surgery.
When to Consult
If diagnosed with ovarian cysts, experiencing pelvic pain, bloating, irregular periods, or suspicious imaging findings.
What to Bring
Ultrasound reports, CA-125 blood test results, HE4 test results, genetic testing (BRCA1/2) if available, and complete gynecological history.
Risk Factors
Causes
Treatment Options
Active Surveillance (Watchful Waiting)
For premenopausal women with simple, small (<5 cm) ovarian cysts and normal CA-125 levels, active surveillance or watchful waiting is the standard approach. Because most functional cysts resolve spontaneously within 8 to 12 weeks, the patient is monitored with a repeat pelvic ultrasound in one to two menstrual cycles to check if the cyst has shrunk or disappeared. Active surveillance avoids the risks of surgery and preserves ovarian tissue. For postmenopausal women, close monitoring with ultrasounds and CA-125 levels is also appropriate for small, simple, asymptomatic cysts.
Hormonal Contraceptives
Hormonal contraceptives, such as oral birth control pills, patches, or vaginal rings, may be prescribed for women who experience recurrent functional ovarian cysts. While hormonal contraceptives do not shrink or treat existing cysts, they work by suppressing ovulation. By preventing the development of new follicles and corpus lutea, they effectively reduce the risk of developing new functional cysts. This treatment is particularly useful for managing symptoms in patients with conditions like Polycystic Ovary Syndrome (PCOS) or recurrent cyst-related pelvic pain.
Laparoscopic Cystectomy (Organ-Preserving Surgery)
For persistent benign cysts, large cysts (>5-6 cm), or complex cysts that cause symptoms, a Laparoscopic Cystectomy is the preferred surgical intervention. Performed under general anesthesia through several tiny keyhole incisions in the abdomen, the surgeon utilizes a laparoscope and specialized instruments to carefully dissect and remove the cyst from the ovary, preserving the remaining healthy ovarian tissue and the patient's fertility. Laparoscopic surgery offers significant benefits over open surgery, including minimal blood loss, less postoperative pain, a lower risk of adhesions, and a rapid recovery time.
Oophorectomy and Salpingo-Oophorectomy
An Oophorectomy (removal of the ovary) or Salpingo-Oophorectomy (removal of the ovary and fallopian tube) may be necessary in certain situations. These include: cases where the cyst is extremely large and has replaced all healthy ovarian tissue; when the ovary has undergone torsion and suffered irreversible tissue death (necrosis); or in postmenopausal women where ovarian preservation is less critical. If there is a high suspicion of malignancy based on imaging and markers, a complete surgical staging procedure including removal of both ovaries, fallopian tubes, uterus, and surrounding lymph nodes is performed.
Frequently Asked Questions
Q. What is the most effective treatment for Ovarian Cysts?
The most effective treatment for Ovarian Cysts depends on the stage, location, molecular profile of the tumor, and the patient's overall health. Dr. R. Srinath Bharadwaj provides personalized protocols including chemotherapy , immunotherapy , targeted therapy , or combination approaches.
Q. Where can I get expert treatment for Ovarian Cysts in Hyderabad?
You can consult Dr. R. Srinath Bharadwaj, a leading Medical Oncologist, at the American Oncology Institute, Nallagandla, Hyderabad. Call +91 91213 36638 to schedule an appointment.
Q. What documents should I bring for a Ovarian Cysts consultation?
Please bring all recent biopsy reports, imaging scans (CT, MRI, or PET-CT), tumor markers, blood test results, and any previous treatment or surgery details to help outline your care plan.