Hairy Cell Leukemia
Specialized treatment for hairy cell leukemia, a rare type of chronic leukemia, with effective chemotherapy options.
Hairy Cell Leukemia
Hematologic Malignancies
Overview
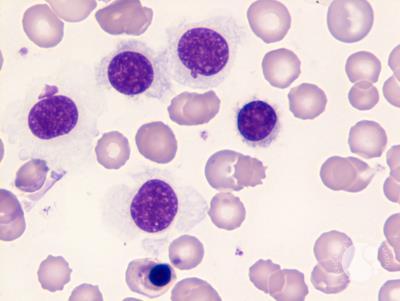
Hairy Cell Leukemia (HCL) is a rare, slow-growing (indolent) B-cell lymphoproliferative disorder, classified as a subtype of chronic leukemia. It is characterized by the accumulation of abnormal, clonal B-lymphocytes in the bone marrow, spleen, and peripheral blood. Under microscopic examination, these leukemic cells exhibit fine, hair-like cytoplasmic projections on their surface, giving the disease its name.
HCL predominantly affects older adults, with a median age of 50 to 60 years at diagnosis, and has a strong male-to-female predominance of approximately 4:1. The accumulation of hairy cells in the bone marrow leads to bone marrow failure, resulting in cytopenias (low blood counts). Specifically, patients develop severe neutropenia (low white cells), anemia (low red cells), and thrombocytopenia (low platelets).
The disease also causes significant infiltration of the spleen, leading to splenomegaly (enlarged spleen), which can grow to massive sizes. Symptoms of HCL include persistent fatigue, weakness, easy bruising or bleeding, recurrent infections (due to neutropenia and monocytopenia), abdominal fullness or pain in the upper left quadrant caused by splenomegaly, and night sweats. A key genetic hallmark of HCL is the presence of the BRAF V600E mutation in nearly all classical cases, which leads to hyperactivation of the RAF-MEK-ERK signaling pathway, driving cell survival and proliferation.
When to Consult
Upon diagnosis of hairy cell leukemia, abnormal blood counts (low platelets, low white cells, anemia), fatigue, infections, or enlarged spleen.
What to Bring
Complete blood count (CBC), peripheral smear, bone marrow biopsy reports, flow cytometry results, BRAF mutation testing, and imaging scans.
Risk Factors
Causes
Treatment Options
First-Line Purine Analog Chemotherapy
Classical Hairy Cell Leukemia is exceptionally responsive to chemotherapy with purine analogs, which are the standard first-line treatment. The primary drug used is Cladribine (2-CdA), administered either as a continuous intravenous infusion over 7 days, daily 2-hour infusions for 5 days, or as weekly subcutaneous injections. An alternative purine analog is Pentostatin, given intravenously every 2 weeks for several months. These drugs are highly effective, achieving complete and durable remission in over 80-90% of patients. Many patients remain in remission for 10 to 15 years or longer after a single course of treatment, offering a near-normal life expectancy.
Monoclonal Antibody Immunotherapy (Rituximab)
Rituximab is a monoclonal antibody that targets the CD20 antigen expressed on the surface of normal and leukemic B-cells. In Hairy Cell Leukemia, Rituximab is used primarily for patients who relapse after purine analog therapy, or in combination with Cladribine (either concurrently or sequentially) to achieve deeper remissions and clear minimal residual disease (MRD) in high-risk patients. By binding to CD20, Rituximab marks the leukemia cells for destruction by the body's immune system, sparing normal tissues and avoiding the typical toxicities of chemotherapy .
Targeted BRAF Inhibitor Therapy
Because the BRAF V600E mutation is the driving genetic alteration in classical HCL, targeted BRAF inhibitors have emerged as a highly effective non- chemotherapy option for patients with relapsed or refractory disease. Oral BRAF inhibitors such as Vemurafenib or Dabrafenib specifically block the mutated BRAF protein, stopping the growth signals in HCL cells. These targeted therapies achieve rapid hematological responses and reduction in spleen size, and are often combined with Rituximab to prolong the duration of remission in patients who have failed multiple prior chemotherapy lines.
Supportive Care and Complication Management
Supportive care is essential during the diagnosis and treatment of Hairy Cell Leukemia, particularly because purine analogs cause transient, severe immunosuppression, increasing the risk of infections. Key measures include: administering prophylactic antiviral (e.g., Acyclovir) and antibacterial/antifungal medications; using granulocyte colony-stimulating factors (G-CSF) to accelerate white blood cell recovery; and monitoring for tumor lysis syndrome. Transfusions of irradiated blood products are provided to treat severe anemia or thrombocytopenia. Long-term surveillance for secondary malignancies is also maintained.
Frequently Asked Questions
Q. What is the most effective treatment for Hairy Cell Leukemia?
The most effective treatment for Hairy Cell Leukemia depends on the stage, location, molecular profile of the tumor, and the patient's overall health. Dr. R. Srinath Bharadwaj provides personalized protocols including chemotherapy , immunotherapy , targeted therapy , or combination approaches.
Q. Where can I get expert treatment for Hairy Cell Leukemia in Hyderabad?
You can consult Dr. R. Srinath Bharadwaj, a leading Medical Oncologist, at the American Oncology Institute, Nallagandla, Hyderabad. Call +91 91213 36638 to schedule an appointment.
Q. What documents should I bring for a Hairy Cell Leukemia consultation?
Please bring all recent biopsy reports, imaging scans (CT, MRI, or PET-CT), tumor markers, blood test results, and any previous treatment or surgery details to help outline your care plan.